The Glasgow Coma Scale (GCS) is the most widely recognized clinical tool used to evaluate consciousness after a brain injury. In emergency medicine and neurology, it serves as a universal language that allows doctors, nurses, and first responders to describe a patient’s level of responsiveness quickly and consistently.
Created in 1974 by Professor Graham Teasdale and Professor Bryan Jennett at the University of Glasgow, the scale transformed how medical teams assess and communicate about brain injury. Before its development, descriptions like “stuporous,” “semi-conscious,” or “deeply comatose” were vague and inconsistent. The GCS introduced a structured, evidence-based scoring system that remains a cornerstone of acute brain injury care across the world.
How the GCS Works
The Glasgow Coma Scale evaluates three core functions of brain activity — eye, verbal, and motor responses. Each provides clues about how different brain regions are performing after trauma.
1. Eye Opening (E)
Eye responses indicate the function of the brainstem and upper midbrain.
- 4: Opens eyes spontaneously
- 3: Opens eyes to verbal command
- 2: Opens eyes to pain
- 1: No eye opening
2. Verbal Response (V)
This measures awareness and language function, reflecting the integrity of the cerebral cortex.
- 5: Oriented and converses clearly
- 4: Confused conversation
- 3: Inappropriate words
- 2: Incomprehensible sounds
- 1: No verbal response
3. Motor Response (M)
This evaluates how well the brain communicates with muscles to follow commands or react to pain.
- 6: Obeys verbal commands
- 5: Localizes pain
- 4: Withdraws from pain
- 3: Abnormal flexion (decorticate posture)
- 2: Abnormal extension (decerebrate posture)
- 1: No motor response
The total score (E + V + M) ranges from 3 to 15, with lower numbers indicating deeper impairment.
| Response Type | Score Range | Key Interpretation |
|---|---|---|
| Eye Opening | 1–4 | Brainstem function |
| Verbal Response | 1–5 | Cortical function |
| Motor Response | 1–6 | Motor pathway integrity |
| Total | 3–15 | Overall consciousness level |
Classifying Brain Injury Severity
The combined GCS score is used to categorize the severity of traumatic brain injury (TBI):
| Total GCS Score | Classification | Description |
|---|---|---|
| 13–15 | Mild TBI | Brief loss of consciousness or confusion; usually good recovery |
| 9–12 | Moderate TBI | Prolonged confusion or unconsciousness; possible neurological deficits |
| 3–8 | Severe TBI | Deep unconsciousness or coma; high risk of long-term disability |
These categories help guide clinical decisions, predict outcomes, and determine what level of monitoring or imaging is needed.
In many hospitals, a GCS score of 8 or below automatically triggers intubation and advanced airway protection, since patients at this level cannot reliably protect their own airway.
Why the GCS Matters in Brain Injury Care
In emergency departments, time is critical. The GCS allows doctors and paramedics to communicate precisely during those first moments — often while stabilizing a patient, ordering imaging, or alerting a trauma team. A quick “GCS 7, E2 V2 M3” tells specialists almost everything they need to know about the patient’s neurological status, even before scans are done.
Beyond its diagnostic value, the GCS also:
- Tracks progress or deterioration over time
- Guides treatment escalation (surgery, ICU care, or rehabilitation)
- Informs prognosis for recovery potential
For families, hearing that their loved one’s GCS has “improved from 6 to 10” provides an early sign of hope.
Using GCS in Children and Infants
The standard GCS is not always suitable for young children who cannot yet speak or follow commands. For this reason, clinicians use the Pediatric Glasgow Coma Scale (PGCS), which adapts verbal and motor criteria to developmental stages.
For example:
- A baby who cries appropriately to pain scores higher than one who is silent.
- Instead of “oriented conversation,” infants are assessed for coos, cries, or appropriate sounds.
This adaptation ensures that children’s neurological function is accurately represented, helping pediatric specialists detect subtle changes in responsiveness.
Limitations of the GCS
Despite its global use, the Glasgow Coma Scale is not perfect. Its accuracy can be influenced by several factors:
- Intubation or tracheostomy, which prevents verbal responses.
- Sedation or anesthesia, which suppresses normal reactions.
- Intoxication, masking neurological function.
- Language barriers or hearing impairment.
- Severe facial or ocular injuries affecting eye responses.
In such cases, clinicians document modified scores — for instance, “E3 V- M5 (verbal not testable)”—and rely on additional assessments such as pupil size, reflexes, and imaging.
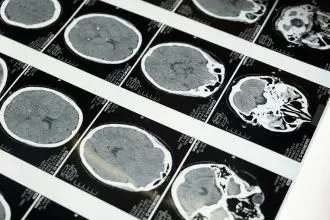
The GCS and Neuroimaging
The GCS is often the first clue that something is wrong, but CT and MRI scans confirm what type of brain injury is present—such as bleeding, swelling, or diffuse axonal injury.
Typically:
- Mild TBI (GCS ≥ 13): A scan may be ordered only if symptoms worsen or there is vomiting, severe headache, or memory loss.
- Moderate to Severe TBI (GCS ≤ 12): CT imaging is mandatory to locate bleeding or pressure buildup that might need surgical intervention.
Thus, the GCS works hand-in-hand with imaging to guide both immediate care and ongoing monitoring.
GCS in the Intensive Care Unit
In critical care, repeated GCS scoring helps track neurological stability. A decreasing score may indicate rising intracranial pressure, new bleeding, or reduced oxygenation. Nurses and neurologists often record GCS scores hourly, alongside pupil reactivity and vital signs, to detect early warning trends.
Even small changes matter; for example, a drop from 11 to 9 may trigger urgent re-evaluation or repeat imaging.
Prognosis and Long-Term Outcomes
Numerous studies link GCS scores with outcome predictions. Patients with higher initial scores generally experience better recovery rates, while those with lower scores may face prolonged coma or severe disability.
However, outcomes also depend on factors like:
- Age and overall health
- Type and location of injury
- Speed and quality of medical intervention
- Access to rehabilitation and follow-up care
For this reason, the GCS is just one part of a larger assessment that includes neuroimaging, neuropsychological tests, and functional evaluations during recovery.
GCS Beyond Traumatic Brain Injury
Although designed for trauma, the GCS is also used in:
- Stroke and intracerebral hemorrhage
- Post-cardiac arrest recovery
- Toxic or metabolic encephalopathies
- Infectious brain diseases like meningitis or encephalitis
Its versatility has made it the international standard for consciousness assessment in virtually every hospital, ambulance, and research setting.
Summary
The Glasgow Coma Scale revolutionized how clinicians assess consciousness and describe brain injury severity. By assigning numerical values to eye, verbal, and motor responses, it provides a clear, objective language for tracking the brain’s function after trauma.
While not a substitute for imaging or neurological exams, the GCS remains the foundation of acute brain injury evaluation. From roadside assessment to ICU monitoring and rehabilitation planning, it continues to save lives and shape decisions, one score at a time.